
INTRODUCTION
Maxillary first molar is a tooth that has been evaluated multiple times for its aberrant anatomy and has been described in the literature for its diversities. Thus, finding an extra canal or an extra root is not something which is a new finding for this tooth. The knowledge of the anatomy of a tooth is an indispensable criterion that decides the success and failure of the endodontic therapy for a tooth. One root, one canal formula is frequently overruled by the fact that number of canals is more than the number of roots. The failure rate of endodontic treatment of maxil- lary molars is high due to the complex morphology of root canals and often missing second mesiobuccal (MB2) and extra canals in distobuccal and palatal root. Moreover, a less than adequate access opening makes it difficult for the primary dentist to locate the supplemental canals.1 The broad buccolingual dimension of the mesiobuccal root and associated concavities on its mesial and distal surface is consistent with the majority of the mesiobuccal roots having two canals.23 Thus, it is of paramount impor- tance for a clinician to have a conscientious knowledge of the tooth being treated so that he can perfectly justify the treatment.
The MB2 canal is not something that is easy to catch. It is usually located either mesial to or in the pulpal groove connecting the main mesiobuccal canal and palatal canals, within 3.5 mm palatally and 2 mm mesially from the main mesiobuccal canal.+6 The incidence of MB2 canal is reported to be between 18 and 96.1%6.7 and the incidence of two canals in the distobuccal root is reported to be between 1.90 and 4.30%. Thus, an operator must always be anticipating. One should look for extra canals because missed canals lead to a decreased long-term prognosis. This case report describes a nonsurgical management of maxillary first molar with two mesial, two distal, and a palatal canal.
CASE REPORT
A21-year-old young male patient reported to the Depart ment of Conservative Dentistry & Endodontics, with the complaint of pain in the upper left back tooth region since last 1 month. History revealed that the pain was moder- ate and continuous in nature and intensified by thermal stimuli and on mastication. The patient’s medical history was noncontributory and unremarkable.
On clinical examination, no sinus was observed. The tooth #26 was tender on percussion with no thermal response and the coronal restoration was incorrectly done. Radiographic examination of the tooth revealed second- ary caries under the composite restoration involving mesial pulp hom, encroaching into the pulp space (Fig. 1).
According to the clinical signs and symptoms, the diagnosis of symptomatic irreversible pulpitis was made and nonsurgical root canal treatment was planned. Res- toration was removed, caries was excavated under 2% local anesthesia in the concentration of 1:200,000, and access preparation was done using #2 and #4 round burs in the beginning followed by Endo Access bur (Dentsply Maillefer, Switzerland). Initial outline form was triangular and three orifices of mesiobuccal, distobuccal, and palatal canals were located following the dentinal map, bleeding points, and a DG16 explorer (Hu-Friedy, Chicago, Illinois, USA). Troughing was performed with the help of an ultrasonic tip (Endosonic, Woodpecker Mectron handpick)
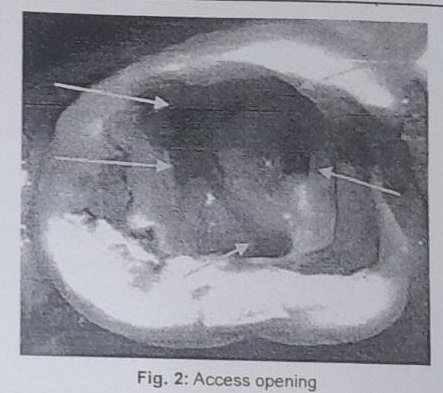
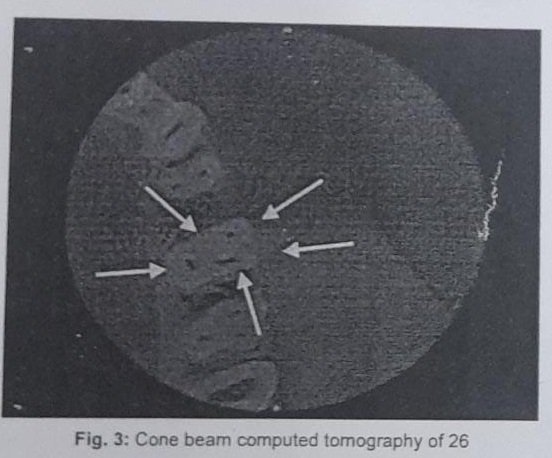
after which MB2 canal orifice was also discovered. At this point, DB2 canal was anticipated and the access opening was further modified to achieve its presence and it was successfully discovered too (Fig. 2). All the canal orifices were enlarged using GG drills. The cone beam computed tomography (CBCT) images confirmed the presence of two more canals palatal to the mesiobuccal and the distobuccal canal orifices (Fig. 3).
The working lengths were determined with apex locater (Propex II, Dentsply Maillefer, Switzerland) and confirmed radiographically (Fig. 4). Cleaning and shaping of canals was done by Crown Down technique using no. 25 K3 nickel-titanium rotary files (SybronEndo, Orange, CA) in a taper of 4%.
About 15% ethylenediaminetetraacetic acid (Dentsply Maillefer Glyde syringe kit) along with 5.25% NaOCl was used to irrigate the canals during instrumentation followed by intermitted irrigation with normal saline.
A preobturation radiograph was taken to confirm that the canal preparation was achieved till the working length (Fig. 5). Canals were then dried with absorbent points
DISCUSSION
Failure of root canal treatment can be attributed to a number of reasons. Inability to identify and negotiate missed canals remains a primary reason for retreatment and can be in as many as 19% of cases.” After gaining access to the pulp chamber, the floor of the chamber must be carefully examined. The dentinal map should be followed and the developmental grooves should be carefully accessed using a DG16 explorer to locate extra canals. The presence of extra canals should not just be anticipated, but they should be meticulously looked for.
Auxiliaries, such as illumination, dental operating microscope, and endodontic loupes serve efficiently to locate extra canals. Yoshioka et al10 demonstrated increased ability to detect and negotiate MB2 when ultra- sonics is used in conjunction with magnification. Gently sweeping the pulpal floor with a slow speed no. 2 or 4 round bur or using an ultrasonic instrument in the same manner aids in finding the extra canals.11 A preoperative two-angled radiograph is also mandatory, especially in the case of maxillary molars. There is superimposition of roots on one another, making radiographic assessment of additional canals impossible on a single projection. The presence of an eccentrically placed file on radio- graph should also raise suspicion of presence of an extra canal. Newer diagnostic methods, such as CBCT help in accessing the internal canal morphology to a great extent. Searching for canal bleeding points, following the dentinal map, staining the pulpal floor with 1% methylene blue dye, and champagne bubble test are another ways to locate extra canal orifices.
CONCLUSION
Even if it is rare, a clinician should always be prepared to encounter any aberrant morphology during an endodon- tic treatment, and should not hesitate to use advanced diagnostic modalities like CBCT for identifying root and canal aberrations in order to ascertain favorable root canal treatment outcomes, while respecting the challenges of pulp space anatomy.14
REFERENCES
1. Tabassum S, Khan F. Failure of endodontic treatment: the usual suspects. Eur J Dent 2016;10(1):144-147.
2. Walton R, Torabinejad M. Principles and practice of endodon- tics. 4th edition. Philadelphia, PA: Saunders; 2002.
3. Nelson S, Ash M, Ash M. Wheeler’s dental anatomy, physiol- ogy, and occlusion. 9th edition; n.d.
4. Cantatore G, Berutti E, Castellucci A. Missed anatomy: fre- quency and clinical impact. Endod Top 2009;15:3-31. 5. Pomeranz HH, Fishelberg G. The secondary mesiobuccal canal
of maxillary molars. J Am Dent Assoc 1974 Jan;88(1):119-124. 6. Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod 1990 Jul;16(7):311-317.
7. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod 2002 Apr;28(4):324-327.
8. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J 1993 Sep;26(5):257-267.
9. Song M, Kim H, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod 2011 Nov;37(11):1516-1519.
10. Yoshioka T, Kikuchi I, Fukumoto Y, Kobayashi C, Suda H. Detection of the second mesiobuccal canal in mesiobuccal roots of maxillary molar teeth ex vivo. Int Endod J 2005 Feb;38(2):124-128.
11. Hartwell G, Appelstein C, Lyons W, Guzek M. The incidence of four canals in maxillary first molars. J Am Dental Assoc 2007 Oct;138(10):1344-1346.
12. Umer F. Maxillary first molar with five canals. Case Rep 2014 Sep,2014:bcr2014205757.
13. Rajalbandi S, Shingte S, Sundaresh K, Mallikarjuna R. Aberra-
tion in the palatal root of the maxillary first molar. Case Rep 2013 Apr 30,2013(1):ber2013008641-bcr2013008641.
14. Shojaeian S, Ghoddusi J, Hajian S. A case report of maxillary second molar with two palatal root canals and a furcal enamel pearl. Iran Endod J 2013,8(1):37-39
Heard pk777game has some cool new features. Thinking about downloading it and giving it a playthrough. Let’s see if it lives up to the hype. Game on: pk777game
Alright! Checking out 511bet. Looks like a contender. Good odds and a decent selection of games. Worth a try I think: 511bet
Gamebet, huh? Never heard of it, but I’m always open to new platforms. Might give it a shot. Anyone else playing there? Learn more here: gamebet.
E aí, pessoal! Encontrei um app novo, o VZ99App. Alguém já usou? Tô procurando um lugar novo para jogar e queria saber se alguém recomenda. Veja aqui: vz99app
Looking to dive into some cockfighting action? Sv388 Login Juraganslot’s got ya covered. Just signed up and it’s pretty straightforward. Check out sv388 login juraganslot.
Anyone tried Go99globe yet? Thinking about checking it out. Seems like a decent option for some online betting. Might give go99globe a punt soon.
Fancy a spin on the roulette wheel, eh? Casinorouletteonline looks like they’ve got a fair few options. Worth a look if you’re after that casino buzz. Check out casinorouletteonline when you get a chance.
phgame https://www.adphgame.net
The Leading Online Casino and Slots Platform in the Philippines visit: jl16login
[9376]Ayala888 Online Casino Philippines: Fast Ayala888 Login, Register, & Slot Games. Secure Ayala888 App Download for the Ultimate Gaming Experience. Experience Ayala888 Online Casino Philippines! Fast ayala888 login, easy ayala888 register, & top ayala888 slot games. Secure ayala888 app download for elite gaming. visit: ayala888