
INTRODUCTION
The increasing demand for aesthetic anterior teeth has always encouraged the practitioners to try newly developed materials for more conservative treatment options. The most conservative treatment alternative of crowded anterior teeth is orthodontic approaches. Nevertheless, orthodontic therapy may be rejected by the patient, due to occupational limitations of time ,cost and appearance during treatment. The potential for orthodontic relapse has inspired the use of tooth preparation and restorative dentistry to recreate tooth dimensions and proportions commensurate with post-orthodontic results from both an aesthetic and functional clinical outcome, thereby eliminating the potential for relapse. With the introduction of adhesive systems, eliminating the need for full coverage for all-ceramic restorations, more conservative treatment options have been put forward. One of the most minimally invasive techniques is application of laminate veneers. Ceramic veneers not only reduce the destructive approach and minimize the gingival reaction risk of full crowns but also mimic the translucency of natural tooth structure.
CASE REPORT
A 22 yr. old male patient reported to Department of Conservative Dentistry & Endodontics with chief complaint of unpleasant looks (while he speaks/ laughs).
Dental history revealed that he got the upper left incisor fractured 3 years back while playing. Presently he had no complain of pain /swelling & totally asymptomatic.
On clinical examination it was found that the upper left incisor was fractured at middle third which had an overlapping relation with adjacent central & lateral incisor.
Radiographic examination revealed that there was small periapical radiolucency associated with the tooth. No root fracture was evident & no significant resorption was seen. Tooth was found to be non vital on performing both thermal &electrical vitality tests.
TREATMENT PLANNING: –
Impressions were taken for both upper & lower arch for one study & two working cast. The dimensions of fractured tooth(21) & adjacent anteriors were taken with the help of divider as follows in cms on the study model.
| TOOTH NO. | 12 | 11 | 21 | 22 |
| DIMESIONS | 0.6 | 0.9 | 0.9 | 0.6 |
1mm from each side (i.e.adjacent central & lateral) without shifting much of midline . Mock preparation was done on 21 for trying to get it in alignment Crown cutting was performed on 21 on first working model & wax patter was
made. on second working model veneer preparation was done. New There were two option as follows:
- To go for full coverage all ceramic crown.
OR
2. Porcelain Veneer.
In the cases which necessitate corrertion or alteration in tooth shape
or position, changes in morphology ceramic veneers display promising esthetic results when clinical procedures carefully carried out. As because of overlapped teeth antagonists (318 32) has come little bucally placed & crown preparation requires reduction from lingual side also. So a veneer was
preferred over crown, As it not only provide esthetic restoration but also conserves the tooth structure which was already lost due to fracture.
TREATMENT PROCEDURE:
The endodontic procedure was performed on 21,root canal was opened, working length was determined with the help of radiograph and the tooth was
obturated Now composite build up was done on 21.. later the tooth was prepared to reduce its labiolingual
dimension to get in alignment with the rest of the arch. It was observed that there was definite decrease in overlapping to a significant amount but not completely.
The preparation was conservative. It allowed space for a coverage of 0.5 mm to 0.75 mm of porcelain. Any area of the tooth that was visually accessible was covered by the porcelain. The margin of the veneer was kept above the gum line. Veneer margins would blend with the gingival enamel and impression making will be easier.
Incisal reduction is an important factor in the long-term fracture resistance of veneers. The incisal edge was reduced
by 1.5 mm and a lingual chamfer was prepared. This chamfer exposes porcelain to compression instead of shearing during the initial phase of protrusive movement, and as long as forces are against the tooth (compressed porcelain), fracture resistance is high.
This procedure confines all the peripheral marginal areas within enamel to ensure adequate sealing
due to better bonding. Final preparations was kept as smooth as possible to improve accuracy of impressions and laboratory procedures. Gingival Retraction cord was placed w.r.t.21.A rubber base impression was made after removing retraction cord .Impression was poured with die stone. A suitable shade was selected under the sunlight with the help of vita 3-D shade guide. The working cast was sent to lab for veneer preparation.
VENEER Cementation:
Veneer was checked for initial adjustment by keeping it on 21. During the cementation process each abutment tooth was etched for 15 s using a 37% phosphoric acid etch-gel. Subsequently the tooth surface was rinsed thoroughly and air-dried gently.
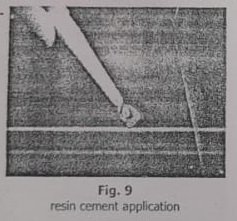
Dentin primer and adhesive were applied according to the manufacturers’ instructions Following the bonding application a thin layer of dual cure composite resin luting cement was applied at the intaglio surface of the veneers, placed onto the prepared teeth
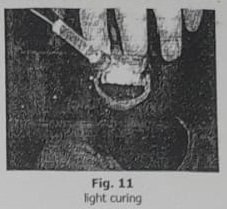
and light-polymerized for 40s from palatal, buccal and incisal sides.
Excess luting cement was removed and the marginal area was finished and polished with abrasive discs and strips. Oxyguard was applied on gingival margins and was left for 3 minutes. The
tooth was air dried & cleaned with cotton.
Restorations were checked to avoid any occlusal interference in both centric &eccentric relation. The patient was
satisfied with his new smile line and excellent view of the anterior teeth. patient was recalled after 2 days and encouraged for better dental flossing. A recall was fixed after 6 months.
Discussion
Esthetics has become a major component of modern dentistry. Orthodontics can be used to facilitate esthetic dentistry in many ways and it is also the most conservative treatment for remodeling the dental appearance and smile. Most patients can benefit functionally
and aesthetically from orthodontic therapy. However, especially adult patients may reject the ornodontic treatment due to Occupational time limitation, appearance during treatment or esthetic and psychological concerns. During the past several decades, the orthodontic alternative has been available for the patients. The most conservative and common method for rehabilitating the problem of malalignment without orthodontic therapy is utilizing ceramic laminate veneers. The goals of therapy
for the orthodontic and restorative dentistry are similar; how they achieve the results is the only difference. On examination patient’s oral hygiene was satisfactory & he was following all measures for maintaining oral hygiene In this case orthodontic treatment was offered to the patient but the suggestion was rejected. The patient had already dental flossing habit, in addition his oral hygiene was satisfactory. Another alternative was suggested to patient by using composite mock-up, but due to low fracture strength and not being as durable and esthetic as ceramics in a dynamic environment like oral cavity direct or indirect composite veneer: could not be planned for this purpose Therefore, porcelain laminate veneer
were optimal solution for the patient. This case presented herein has replicated the treatment outcomes of orthodontic therapy through the use of aesthetic and restorative techniques. Ceramic veneers displayed promising
results when considering the esthetic and mechanic criteria’s. The adoption of non-invasive methodology during aesthetic treatment is in agreement with not only ethical considerations but also physiological ones. By using non- invasive porcelain veneers, we are able to enhance the smile of patients, with a completely reversible approach, without removing any of their natural tooth structure and therefore with no
interference with the physiology of their teeth. Owing to the presence of enamel under the whole fitting surface, bonding procedures are very strong crowded teeth by modifying stone models. J Esthet Restor Dent. 2001;13(1):29-39. and the flexural properties of the 7. Wootipoom N.: [Porcelain laminate underlying natural teeth are also unchanged; thus, they are expected to last for many years.
Conclusion
Naturally, non-invasive methodology cannot always be adopted because of various clinical situations and treatment demands. Nevertheless, whenever possible, additive procedures should be preferred to resectional ones.
REFERENCES:
1. PATHWAYS OF PULP: COHEN,9TH EDITION.
2. TEXTBOOK OF ENDODONTICS INGLE,6″ EDITION.
3. ENDODONTIC THERAPY: WIENE,6″ EDITION.
4. TEXTBOOK OF PROSTHODONTICS : ROSENSTEIL.
5. ENDODONTICS: GROSSMAN, 11TM EDITION.
6. Cutbirth ST: Treatment planning for porcelain veneer restoration of crowded teeth by modifying stone models Esthet Restor Dent. 2001;13(1): 29-39.
7. Wootipoom N.: [ Porcelain laminate ] veneers: a conservative esthetic treatment. Report of 3 cases J Dent Assoc Thai. 1990 Sep- Oct;40(5):203-9. Thai
8. Nalbandian S, The effect of veneers on cosmetic improvement Br Dent J. 2009 Jul 25;207(2):E3; discussion 72-3
9. Chander NG: Finite Element Stress Analysis of Diastema Closure with Ceramic Laminate Veneers J Prosthodont. 2009 Jun 11. [Epub ahead of print]
10. Chu FC.: Clinical considerations in managing severe tooth discoloration with porcelain veneers. J Am Dent Assoc. 2009 Apr;140(4):442-6.
11. Cho MS: Opalescence of all- ceramic core and veneer materials Dent Mater. 2009 Jun;25(6):695- 702. Epub 2009 Jan 14.
12. Lampreia : Aesthetic porcelain laminate veneer restoration following orthodontic treatment: sequential technique, Pract Proced Aesthet Dent. 2008 Oct;20(9):545-7.
If you’re looking to enhance your smile, ceramic veneers in Mira Bhayandar can give you amazing results.
Got ceramic veneers in Mira Bhayandar amazing results, expert care, and a smile transformation.
Ceramic veneers in Mira Bhayandar gave me the perfect smile, great service, and a flawless finish.
Interesting analysis! Seeing how patterns emerge is key, and tools like the Nano Banana Generator could really help visualize those trends. Accessible tech is a huge plus too – web-based platforms are so convenient!
Alright, time to give jili711casino a spin! I’ve heard some rumblings. Hopefully they pay out. Putting my luck to the test! Check it out for yourself jili711casino!
Alright, gave 2phcasinologin a spin. Just your average online casino experience, if you ask me. If you enjoy those, then knock yourself out. Don’t lose the rent money now, okay? Check it out here: 2phcasinologin
Just signed up for 789win1vip. The VIP treatment sounds pretty sweet, fingers crossed it lives up to the hype. Lots of games to play so far! Take a look at 789win1vip!
881bet login was smooth, no issues there. Pretty standard process, like most other sites. If you’re looking to try something new, this login experience won’t be a headache. 881bet login
I am thanksful for this post!
q25casino https://www.laq25casino.com
galaxybet https://www.playgalaxybet.net
phlbest https://www.phphlbest.org
Milyun88: Slot Gacor, Login & Daftar – Link Alternatif Resmi & Download APK Milyun88 Philippines Experience the best milyun88 slot gacor at Milyun88 Philippines. Access our official milyun88 login, milyun88 daftar, and milyun88 link alternatif. Download milyun88 apk and start winning today! visit: milyun88
So, gk999bet… I hopped on, placed a few bets, and had a good time. The interface is clean and easy to use, which is a big plus. Maybe luck will be on your side when you visit gk999bet
Stumbled upon bl888 the other day. Seems like a cool resource. Definitely worth bookmarking for future reference. Check out what everyone’s talking about over at bl888!
Been playing tt88nohu for a week now, and honestly, I’m hooked! It’s super engaging and keeps me coming back for more. Give tt88nohu a try—you might get addicted too!
C99game? It’s not bad. It’s pretty basic, and honestly the gameplay is as expected. Good if you want something not hard to pick it up! Have a look at c99game.
Yo, just grabbed the i777gamedownloadapk, and it’s legit! Downloading games is a breeze. Check it out i777gamedownloadapk for some serious fun.
Trying my luck with 4playbetlogin tonight. The login was smooth, and the interface looks clean. Let’s see if I can win something big! Give it a shot 4playbetlogin.
Hey, I’ve been checking out rss99game lately and it’s pretty cool. The games load fast and they’ve got a decent selection. Definitely worth a look if you’re looking for something new online. Check it out at rss99game
Just tried upbet1 and gotta say, I’m impressed. Smooth interface and easy to navigate. Seems like a solid platform for betting, give upbet1 a try!
Yo, vando88 is where it’s at. Good odds and a nice variety of options. Been having some fun there, check out vando88 if you’re looking to spice things up.
[4111]Casinoplusph Official Website: Easy Login & Register for the Best Online Slots in the Philippines. App Download available for 24/7 gaming! Experience the best online slots at the Casinoplusph official website. Quick Casinoplusph login & register for top PH gaming. Get the Casinoplusph app download now! visit: casinoplusph